
Here is a physiotherapists outlook on common running injuries and the long term effects of them based on research available here, here and here.
DO YOU SUFFER FROM PAIN OR DISCOMFORT DURING OR AFTER RUNNING? |







 | 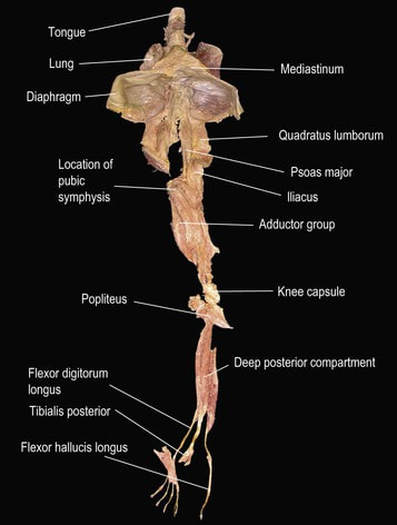 |
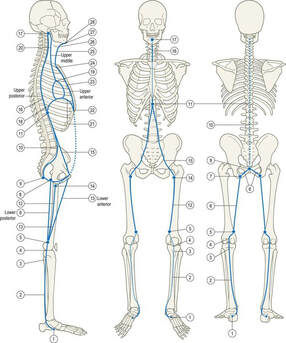
| Though DFL is present throughout your body, for convenience, let’s describe it from your foot. DFL begins from the deep of the foot. Distal attachments of muscles in the back of the foot namely: the tibialis posterior and the two long flexors of the toes, the flexor hallucis and, digitorum longus mark the beginning of DFL. From there, DFL passes inside the ankle behind the medial malleolus. From there DFL moves towards the deep posterior compartment of the lower leg, behind your knee and then moving towards the thigh. From there, a major branch of DFL passes by the front of your hip joint, pelvis, and lumbar spine. | A horizontal cross-section of meridians in your leg: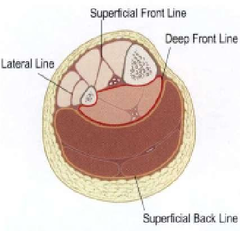 |
From your thigh, another branch of DFL reaches the floor of the pelvis and from there goes up to your lumbar spine and joins the major branch of DFL there. From lumbar spine, DFL moves above through your ribcage. Few branches of DFL, also surround the rib cage. Thus, DFL reaches the base of your brain.
| Here are top 5 functions of DFL
|  |
Any issue with DFL may result in the following
 |
|
Functions of DFL elaborated
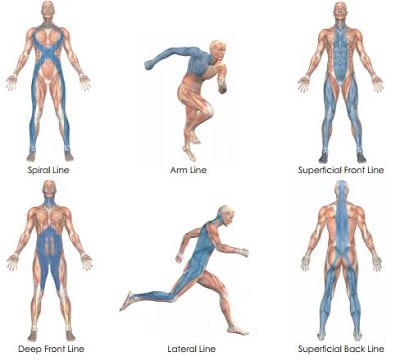
DFL is responsible for the right shape/ position of legs, which create an appropriate inner arch. DFL and Lateral Line/ LL act in reverse directions. The lateral line is a myofascia which begins from the foot and runs on the side of the body. DFL and LL counteract each other. For instance, if DFL falls short around the ankle, the feet turn supine and inverted, whereas if LL gets shorter over a period of time, feet get everted and pronated. Together DFL and LL stabilise tibia and fibula over the ankle and maintain the inner arch.
At the knee joint, DFL and Lateral Line/ LL counterbalance each other like a bowstring. If DFL is short, legs are in the O pattern, and LL is under stress, whereas in the X shaped legs/ knock knees, it’s the other way which means LL is short and DFL is strained.
If there is pain or an imbalance work with your physio to correct this to be able to function without pain.
The good news is that these things can be corrected with the right treatment and exercises!
At the knee joint, DFL and Lateral Line/ LL counterbalance each other like a bowstring. If DFL is short, legs are in the O pattern, and LL is under stress, whereas in the X shaped legs/ knock knees, it’s the other way which means LL is short and DFL is strained.
If there is pain or an imbalance work with your physio to correct this to be able to function without pain.
The good news is that these things can be corrected with the right treatment and exercises!
References:
Findley, T. (2009) Second International Fascia Research Congress. International Journal of Therapeutic Massage & Bodywork: Research, Education, & Practice. 2(2) pp. 1-6.
Ingber, D. (2006) Cellular mechnotransduction: putting all the pieces together again. The Federation of American Societies for Experimental Biology. 20 pp. 811-827.
1 Juhan, D. (2003) 3rd ed. Job’s Body. Station Hill Press, Barry Town, USA.
Myers, T. (2009) 2nd ed. Anatomy trains. Edinburgh: Churchill Livingstone Elsevier. & www.anatomytrains.com
Levin, S. & Martin, D. (2012) Biotensegrity. in Schleip, R., Findley, T., Chaitow, L. & Huijing, P. (eds.) Fascia, the tensional network of the human body. Edinburgh: Churchill Livingstone Elsevier.
https://www.anatomytrains.com
https://www.functionalpatterns.com
https://www.ncbi.nlm.nih.gov/pubmed/11780782
http://healingartsce.com/advancedanatomymyofascialpg4.html
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4107879/
https://www.pilates.org.au/myofascia/#
https://www.pilates.org.au/about/
http://www.psmgroup.com.au/what-is-myofascia
Ingber, D. (2006) Cellular mechnotransduction: putting all the pieces together again. The Federation of American Societies for Experimental Biology. 20 pp. 811-827.
1 Juhan, D. (2003) 3rd ed. Job’s Body. Station Hill Press, Barry Town, USA.
Myers, T. (2009) 2nd ed. Anatomy trains. Edinburgh: Churchill Livingstone Elsevier. & www.anatomytrains.com
Levin, S. & Martin, D. (2012) Biotensegrity. in Schleip, R., Findley, T., Chaitow, L. & Huijing, P. (eds.) Fascia, the tensional network of the human body. Edinburgh: Churchill Livingstone Elsevier.
https://www.anatomytrains.com
https://www.functionalpatterns.com
https://www.ncbi.nlm.nih.gov/pubmed/11780782
http://healingartsce.com/advancedanatomymyofascialpg4.html
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4107879/
https://www.pilates.org.au/myofascia/#
https://www.pilates.org.au/about/
http://www.psmgroup.com.au/what-is-myofascia
And why health or fitness ‘professionals” give out the wrong information.
Hamstring tightness (or any type of single muscle tightness) is being thrown around the web as being the way to cure back pain, knee pain, ankle pain etc. If your hamstrings are shortened then lengthening them may be part of process of relieving your pain; however if this muscle is normal length or long then this may add to your dysfunction and long term may cause a small injury to become a large one.
This common misconception that there is a quick fix for everything is one that is becoming more and more common. Embarrassingly to me this is being led by both health and fitness specialists who give blanket information to everyone to try to boost their social media following to make more money!
This common misconception that there is a quick fix for everything is one that is becoming more and more common. Embarrassingly to me this is being led by both health and fitness specialists who give blanket information to everyone to try to boost their social media following to make more money!
Why is this incorrect?
Lets start by addressing the basic principles and then the anatomy.
Basic Principle 1
Our skeleton is moved by a system of muscles, ligaments and fascia. It uses lots and lots of pulleys to do this. This is an example of a simple 2D pulley.
As seen below the load is affected by gravity:
Basic Principle 1
Our skeleton is moved by a system of muscles, ligaments and fascia. It uses lots and lots of pulleys to do this. This is an example of a simple 2D pulley.
As seen below the load is affected by gravity:
A simple pulley system
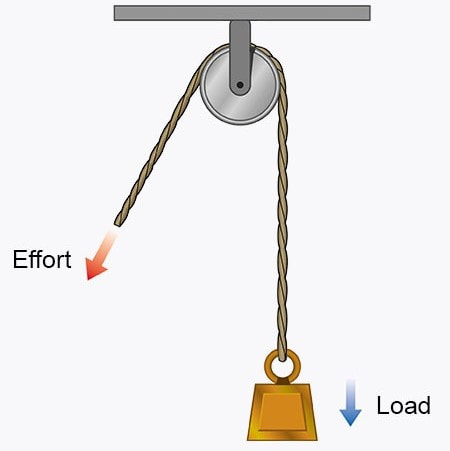
When you pull the rope labelled 'effort' the load moves against gravity.
Basic anatomy...
I promise to be simple
The hamstring group attaches (anchor point) to the back of the pelvis and then travels down the back of the leg and attaches (anchor point) below the knee:
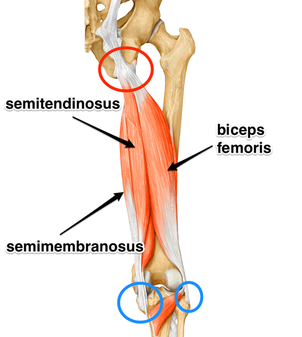
Often the hamstrings feel “tight” or “short” when in reality the pelvic position is just giving us this illusion as we have moved one of the anchor points away putting that muscle on stretch, as seen below:
| NEUTRAL PELVIS POSITION (correct) | ANTERIOR PELVIC TILT (incorrect) |
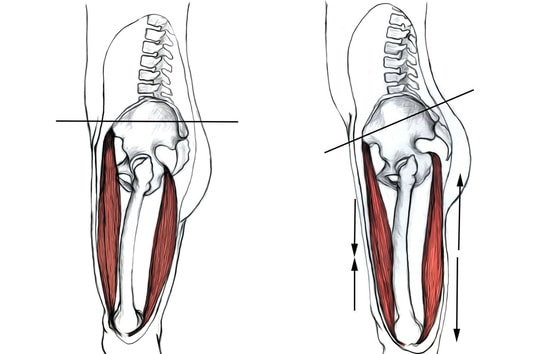
| | Front of body | Back of body | |
As mentioned in my rant about posture retraining we know the body adapts to mechanical forces that cause stress to be placed on the body. In this example we have a lengthening force applied on the hamstring and a shortening force applied on the hip flexor and quad complex causing a stress. This will cause adaptation. As seen above you can also notice that the low back (lumbar spine) is then placed in an extended position and a mechanical force is placed upon the spine leading to adaptation.
Please don’t stretch things that aren’t shortened and if you are unsure please seek a professional’s help that you trust...
...And If you are not getting change its probably the wrong treatment.
Please don’t stretch things that aren’t shortened and if you are unsure please seek a professional’s help that you trust...
...And If you are not getting change its probably the wrong treatment.
Sean Yates | Physiotherapist | Doctor of Physiotherapy | Bachelor of Exercise Science |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
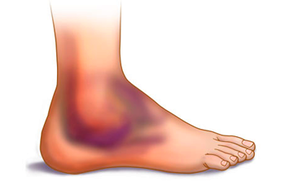
Is my Ankle Rolled or Broken?
 |  |
We have all rolled our ankle at some stage in our life but how do we know if it is more than just a very mild sprain?
Every year in Australia, hundreds of thousands of people visit the emergency room with ankle injuries.
Of these, the majority are sprains and fractures, and in many cases, it can be hard to tell the two apart at first.
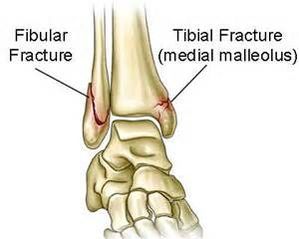
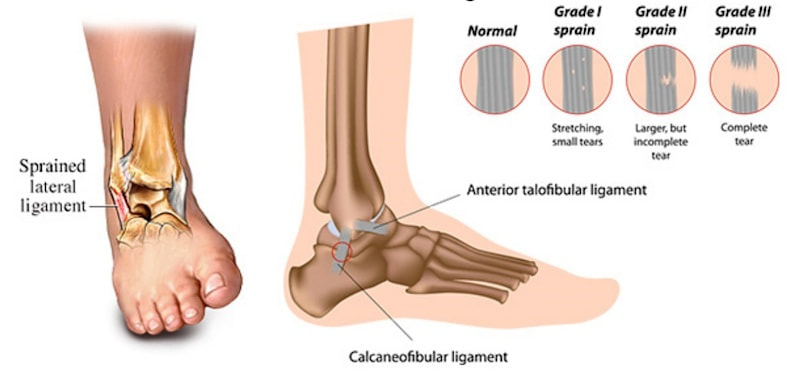
While a fracture refers to a break in one or more of the ankle bones (tibia, fibula, talus or calcaneus), a sprained ankle refers to damage to the ligaments of the ankle due to overstretching beyond their normal range of motion.
Every year in Australia, hundreds of thousands of people visit the emergency room with ankle injuries.
Of these, the majority are sprains and fractures, and in many cases, it can be hard to tell the two apart at first.
While a fracture refers to a break in one or more of the ankle bones (tibia, fibula, talus or calcaneus), a sprained ankle refers to damage to the ligaments of the ankle due to overstretching beyond their normal range of motion.
Both of these conditions can be very painful and occur as a result of similar injuries, but may require a very different management. Some of the most common causes of ankle pain include sports injuries, walking on uneven surfaces and car accidents. So, with the symptoms being so similar, how can you tell a broken or sprained ankle apart? The Ottawa Ankle rules are the best predictor of requiring X-rays.
The other indications with your ankle having something more serious wrong with it are
if there was a sound when you were injured. A “cracking” noise may be a sign that the ankle is broken while sprains may be associated with a “popping” sound. Second, check if the ankle appears deformed or crooked in addition to being swollen as this may be a sign of a fracture.
Third, the presence of numbness is indicative of a fracture. Moreover, if you cannot move the ankle joint at all, are in extreme pain, and cannot put any weight at all on the ankle, it is likely that it is broken.
To be sure, it is important that you have a thorough physical examination by a health professional specialising in the musculoskeletal system. (this should include looking for bony tenderness as well as multiple special tests, This is usually done by a physiotherapist, a sports doctor or surgeon, If warranted further scans may requested including an X-ray, an MRI, a CT or an ultrasound.
If, after 24- 48hours your pain is not getting better or getting worse or your swelling is not getting better or getting worse please seek a health professional in your area.
Sean Yates | Physiotherapist | Doctor of Physiotherapy | Bachelor of Exercise Science |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
if there was a sound when you were injured. A “cracking” noise may be a sign that the ankle is broken while sprains may be associated with a “popping” sound. Second, check if the ankle appears deformed or crooked in addition to being swollen as this may be a sign of a fracture.
Third, the presence of numbness is indicative of a fracture. Moreover, if you cannot move the ankle joint at all, are in extreme pain, and cannot put any weight at all on the ankle, it is likely that it is broken.
To be sure, it is important that you have a thorough physical examination by a health professional specialising in the musculoskeletal system. (this should include looking for bony tenderness as well as multiple special tests, This is usually done by a physiotherapist, a sports doctor or surgeon, If warranted further scans may requested including an X-ray, an MRI, a CT or an ultrasound.
If, after 24- 48hours your pain is not getting better or getting worse or your swelling is not getting better or getting worse please seek a health professional in your area.
Sean Yates | Physiotherapist | Doctor of Physiotherapy | Bachelor of Exercise Science |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
COREman misconceptions
Why your core is soooooo important
Lets start off by getting to the “CORE” of this issue.
When I ask close to 90% of clients I treat to tell me what the core is they can’t, and this makes it hard to understand what the core actually does.
When I ask close to 90% of clients I treat to tell me what the core is they can’t, and this makes it hard to understand what the core actually does.
So what exactly is the "core"
The core is a group of muscles that provide stability to the axial Skelton.
Major muscles included are (in order of approximate depth of the body/closeness to the body’s core):
Major muscles included are (in order of approximate depth of the body/closeness to the body’s core):
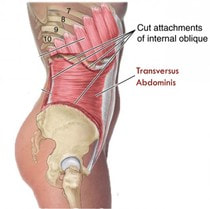
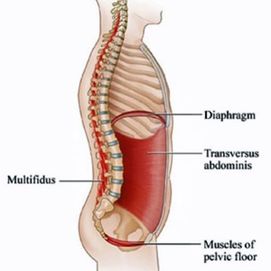
- Transversus abdominis (TvA)
- The pelvic floor muscles
- The diaphragm.
- Internal and external obliques
- Multifidus
- Erector spinae group (ESG). Sacrospinalis and the longissimus thoracis
- Rectus abdominis
- Minor core muscles include the latissimus dorsi, gluteus maximus, and trapezius (but these are also have primary roles in locomotion)
What does Transverse Abdominus do?
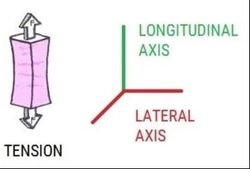
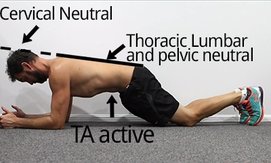
Transverse Abdominus has multiple roles but its primary role is stability. If we define stability as the ability to limit displacement and maintain structural integrity. The TvA, when used correctly (along with primarily the pelvic floor and diaphragm muscles) provide intra-abdominal pressure which helps to provide a longitudinal force on the spine, pelvis and trunk(Figure 1.2).
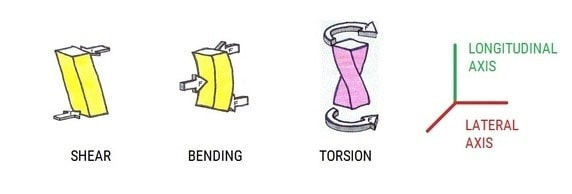
We can assume that, core stability can be defined as the ability of the Thoraco-lumbopelvic-hip complex to prevent shear, bending and torsional forces to cause damaging or buckling such as (kyphosis, Lordosis or scoliosis) of the vertebral column and return it to equilibrium (neutral) following perturbation (external forces).
We can assume that, core stability can be defined as the ability of the Thoraco-lumbopelvic-hip complex to prevent shear, bending and torsional forces to cause damaging or buckling such as (kyphosis, Lordosis or scoliosis) of the vertebral column and return it to equilibrium (neutral) following perturbation (external forces).
If you aren't sure about how to use your core please don't hesitate to contact us
What happens when we don’t use our core?
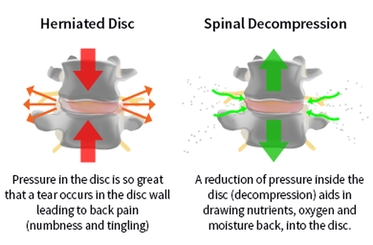
As mentioned before our core provides a longitudinal force on our entire torso. This is very important as gravity (along with the ground reaction force) also provides a longitudinal force in the opposite direction.
Because of the TvA fibre direction it is the only muscle able to provide tension or decompression to the lumbar spine.
Multiple studies have look at the core and its relationship to injury and lower and upper body function, and have all come up with the same conclusions such as decreased core stability may predispose to injury and that appropriate training may reduce injury.
Participants with chronic LBP receiving motor control exercise had a greater improvement in recruitment of transversus abdominis (7.8%) than participants receiving general exercise (4.9% reduction) or spinal manipulative therapy (3.7% reduction).
There was a significant, moderate correlation between improved recruitment of transversus abdominis and a reduction in disability specific training by physical therapy in the raising of the intra-abdominal pressure as a protection for the spine might be of great benefit to patients recovering from “ slipped disc “ or operations upon the spine.
Because of the TvA fibre direction it is the only muscle able to provide tension or decompression to the lumbar spine.
Multiple studies have look at the core and its relationship to injury and lower and upper body function, and have all come up with the same conclusions such as decreased core stability may predispose to injury and that appropriate training may reduce injury.
Participants with chronic LBP receiving motor control exercise had a greater improvement in recruitment of transversus abdominis (7.8%) than participants receiving general exercise (4.9% reduction) or spinal manipulative therapy (3.7% reduction).
There was a significant, moderate correlation between improved recruitment of transversus abdominis and a reduction in disability specific training by physical therapy in the raising of the intra-abdominal pressure as a protection for the spine might be of great benefit to patients recovering from “ slipped disc “ or operations upon the spine.
Now for my Rant!

Transverse Abdominus creates stability using tensegrity or biotensegrity to be precise. This is defined by Kenneth Snelson, to indicate that the integrity of the structure derived from the balance of tension members, not the compression struts.

In lamens terms you can use the analogy that our bodies behave like a suspension bridge (they are able to disperse external forces such as when a large storm causes movement but not cracking), as opposed to a house or stone arch , which is built on compression and has no movement properties.

I am about to make some assumptions but before that I will tell you them I want to share what findings I will base them on.
What we know:
Transvere abdominus is innervated by the intercostal nerves (arising from nerve roots T7-11) and the iliohypogastric nerve and the ilioinguinal nerve (L2-4)
TvA roles are to:
It is common knowledge muscles can work concentrically, eccentrically and isometrically.
I am going to make an assumption here that muscles can do more than one thing at once.
We know that Synergists act together to produce or control a movement (eg the hamstring complex and the gastrocnemius muscle act along with certain fibres of adductor magnus to produce knee flexion, inhibit anterior translation of the tibia on the femur, while maintaining knee positioning through range in the coronal, sagittal and frontal planes.
So why shouldn’t your core be able to do all those things?
Pain is very rarely (I am going to stick my neck out here and say never) a single muscle or structure issue. However a lot of research tends to lean towards the changes of TvA being constant while other musculature is not.
Some more recent research suggests that pain maybe linked to overuse of superficial muscle activation and that training of bilateral activation is an effective training stimulus to change the way the muscle is activated in function, despite the fact that this may not be the only way it is active in function. This principle of a training stimulus that does not reflect every function is true for many exercise approaches.
Transvere abdominus is innervated by the intercostal nerves (arising from nerve roots T7-11) and the iliohypogastric nerve and the ilioinguinal nerve (L2-4)
TvA roles are to:
- Stabilise the thorax and pelvis during dynamic movements
- Without a stable spine (proper contraction of the TvA) the nervous system is inhibited in providing correct recruitment to peripheral muscles this will inhibit the body to perform these functions or functional activities correctly (eg. Standing, walking, running, throwing, lifting, jumping).
- Provide intraabdominal pressure
- Originates most if not all of the body’s functions
- Return the body to a position of neutral when acted upon by an external, or internal force
- Provides static core functionality to resist
- Gravity
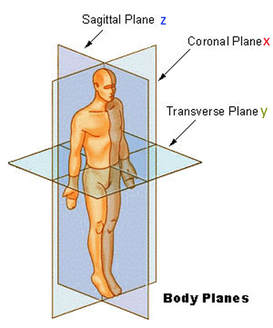
- Produce movement and resist movement in all planes of motion (transverse [head to toe], sagittal [left to right], and coronal [ front to back]
It is common knowledge muscles can work concentrically, eccentrically and isometrically.
I am going to make an assumption here that muscles can do more than one thing at once.
- We have proven that TvA is:
- Active in trunk rotation (greater with contralateral rotation initially but by the time movement starts it has evened out)
- Active with walking (greater with heel strike)
- Active in breathing
- Active with arm movements
We know that Synergists act together to produce or control a movement (eg the hamstring complex and the gastrocnemius muscle act along with certain fibres of adductor magnus to produce knee flexion, inhibit anterior translation of the tibia on the femur, while maintaining knee positioning through range in the coronal, sagittal and frontal planes.
So why shouldn’t your core be able to do all those things?
Pain is very rarely (I am going to stick my neck out here and say never) a single muscle or structure issue. However a lot of research tends to lean towards the changes of TvA being constant while other musculature is not.
Some more recent research suggests that pain maybe linked to overuse of superficial muscle activation and that training of bilateral activation is an effective training stimulus to change the way the muscle is activated in function, despite the fact that this may not be the only way it is active in function. This principle of a training stimulus that does not reflect every function is true for many exercise approaches.
My Summary
The core is a very important group of muscles its primary role is to provide tensegrity to the trunk to allow the peripherals to move off a tensed structure not compressed. Without correct TvA is you will not be able to produce a longitudinal/decompressive force on your spine and trunk. Compression leads to forces such as shear, bending or torsion. If these are done in a controlled manner then the elastic properties of the soft tissue will not adapt however if this is sustained creep or distortion becomes a big problem.
The actual numbers of force through the spine
Discs have a yield (point before permanent damage is done) of between 150 and 600 kgs of force. To put that into perspective I will quote directly with lb to kg conversion in brackets) from a study done.
“A weight of 100 pounds (45kgs) acting on the long lever is only a modest representation of what actually can be lifted by a strong man ; and to this weight should be added the weight of head and shoulders. Let the lever be only fifteen inches, but let us assume that he lifts 200 pounds (90kgs) plus fifty pounds (head, shoulders and thorax), then the pressure in the lumbo-sacral disc will be 2,000 pounds (910kgs). This calculation is based upon stationary forces. And not dynamic ones. The calculation for force is Force = mass time accereration (F= ma). This is important to realise that the acceleration and deceleration forces multiply (not adds) to the total force on the spine.
The pressures that appear during violent action according to this reasoning must be considerably higher and can only be characterised as enormous.
Without correct core you should not be lifting heavy or fast
PLEASE EXCERCISE WITH TRANSVERSE ABDOMINUS ACTIVATION TO DECOMPRESS YOUR SPINE AND MINIMISE INJURY RISK
“A weight of 100 pounds (45kgs) acting on the long lever is only a modest representation of what actually can be lifted by a strong man ; and to this weight should be added the weight of head and shoulders. Let the lever be only fifteen inches, but let us assume that he lifts 200 pounds (90kgs) plus fifty pounds (head, shoulders and thorax), then the pressure in the lumbo-sacral disc will be 2,000 pounds (910kgs). This calculation is based upon stationary forces. And not dynamic ones. The calculation for force is Force = mass time accereration (F= ma). This is important to realise that the acceleration and deceleration forces multiply (not adds) to the total force on the spine.
The pressures that appear during violent action according to this reasoning must be considerably higher and can only be characterised as enormous.
Without correct core you should not be lifting heavy or fast
PLEASE EXCERCISE WITH TRANSVERSE ABDOMINUS ACTIVATION TO DECOMPRESS YOUR SPINE AND MINIMISE INJURY RISK
Something to ponder
The Human and mammal trunk is separated by the diaphragm. The position of the Lungs inside the thoracic cavity (outside the intraabdominal pressure) is an obvious advantage in the evolutionary process. In our situation breathing can occur even when the core is turned on and used as a support and cannot be relaxed. This means that range of flight (ability to work at an aroused level) of an animal having the lungs outside the “core” greater than that of an animal who has its lungs in the single body cavity, which can just make a spurt and then has to stop to breathe.
Could it be that it is for this reason that the mammals have developed a diaphragm?
Why are you holding your breath when you exercise?
#alwayslearning #physiolabs #humanmovement #humanevolution #core #posture #TvA #functionalpatterns #functionalpatternsqueensland #functionalpatternsgoldcoast #lifting
Could it be that it is for this reason that the mammals have developed a diaphragm?
Why are you holding your breath when you exercise?
#alwayslearning #physiolabs #humanmovement #humanevolution #core #posture #TvA #functionalpatterns #functionalpatternsqueensland #functionalpatternsgoldcoast #lifting
Sean Yates | Physiotherapist | Doctor of Physiotherapy | Bachelor of Exercise Science |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
ASCA level 1 | AWF Level 1 coach | Functional Patterns Level 1, 2, 3 | Human Biomechanics Specialist | Dry Needling | Clinical Pilates Level 1, 2, 3 | APA sports Level 1 | Watson Headache Level 1 | IASTM - Smart Tools Instructor |
STARTING YOUR CAREER

You’ve been offered a job and it seems great, you are extremely excited to start your career as a physiotherapist. Before getting ahead of yourself, it is important to be diligent before signing a contract. How does the company want to structure your position – as an employee or an independent contractor?
Employee
Usually reserved for larger, more established practices and government positions.
Pros:
Cons:
Pros:
- Stability in work and pay/ job security
- Structured mentorship
- Leave entitlements
- Industrial relation protections
- Employee benefits
Cons:
- Lack of flexibility in schedule
- Package may be structured differently
- Less flexibility to take on other work

Independent Contractor
Being hired as an employee is straightforward for most graduates, so we will focus on the independent contractor side of the business, since many positions in private practice function this way.
As an independent contractor you have the right to decide where, when and how your work is done. This is extremely important to remember. With the added risk of being self-employed, you gain the flexibility in your schedule and hours.
To check whether the terms of your contract mean indicate that you are an employee or a contractor please visit the ATO calculator here and contact the fair work ombudsman here.
TIP: Before accepting a position and starting your career, it is highly suggested that you shadow another physiotherapist at the clinic during a busy day.
This is good for two reasons:
If you sense an unfriendly atmosphere, an inefficient clinic operation, or a lack of patient traffic, don’t assume it will change once you accept the position. Unfortunately, building a full caseload takes a lot of time and effort, and the location and reputation of the clinic plays a large role in the amount of new patients that walk through the door. Don’t expect to start off extremely busy right away as a new grad until you build your reputation as a clinician. Also, the time of year you start your career will impact how busy you will be. Many physiotherapy clinics have slow periods, such as right after the holidays and during the summer months. Also, there will be many days where a patient will not show up for an appointment or will cancel at the last minute. Remember, as an independent contractor, you only get paid when seeing a patient.
As an independent contractor you have the right to decide where, when and how your work is done. This is extremely important to remember. With the added risk of being self-employed, you gain the flexibility in your schedule and hours.
To check whether the terms of your contract mean indicate that you are an employee or a contractor please visit the ATO calculator here and contact the fair work ombudsman here.
TIP: Before accepting a position and starting your career, it is highly suggested that you shadow another physiotherapist at the clinic during a busy day.
This is good for two reasons:
- To observe the flow and atmosphere of the clinic
- To observe the amount of patient traffic
If you sense an unfriendly atmosphere, an inefficient clinic operation, or a lack of patient traffic, don’t assume it will change once you accept the position. Unfortunately, building a full caseload takes a lot of time and effort, and the location and reputation of the clinic plays a large role in the amount of new patients that walk through the door. Don’t expect to start off extremely busy right away as a new grad until you build your reputation as a clinician. Also, the time of year you start your career will impact how busy you will be. Many physiotherapy clinics have slow periods, such as right after the holidays and during the summer months. Also, there will be many days where a patient will not show up for an appointment or will cancel at the last minute. Remember, as an independent contractor, you only get paid when seeing a patient.
More common in smaller physiotherapy clinics and small-medium sized companies.
Pros:
Pros:
- Flexibility in schedule and place of work
- Can deduct business expenses
- Less stability in your job
- Have to budget for income tax
- No benefits/employee entitlements (eg. Leave)
Negotiating Pay
Due to the lack of: benefits, job security, vacation, holiday pay, bonuses, and consistent work hours, independent contractors usually receive a higher percentage of billings. As a new graduate, your pay will likely be structured as a fee for service. This model means you are only getting paid when you see a patient. Typically the fee split is percentage based and can range from 35-50%. New graduates normally receive a lower percentage to start. Percentage will increase with experience, continuing education courses, and negotiation skills.
| To determine if you are receiving fair pay compared to an employed physiotherapist position, it is helpful to consider a few variables and run the numbers:
|  |
Employee Benefits
| Employee cost is the cost to the employer of hiring an employee instead of an independent contractor. Typically, an employee will cost the company ~25% more. This is due to:
|  |
In general, an independent contractor should charge 20-30% more for their services compared to a full-time employee. Therefore, if you could accept a position in a clinic at $20/hour as an employee, an independent contractor should be paid $26/hour (i.e. 30% more) for that same position to be in the same position financially.
CLICK HERE FOR OUR
NEW GRAD GUIDE TO PRIVATE PRACTICE PHYSIOTHERAPY 1

Are you a new graduate or an AHPRA registered internationally trained physiotherapist looking to enter private practice?
FINDING A JOB
You’ve written the exam, and you’ve practiced and performed the practical exam. Now it’s time to venture into the real world and start looking for work.
Where do you find positions?
Where do you find positions?
It’s not what you know, it's who you know
Fortunately, or unfortunately for some, physiotherapy is a relationship and rapport building profession. The first step to finding a job that is suited to you is to reach out to your contacts, whether they are classmates, former students, clinical instructors or friends. A quick phone call is best, otherwise an email stating that you are looking for work may have you landing your first job before you know it.
The world is at your fingertips:The internet is everywhere these days and this will be the most common avenue to find a position. When you aren’t working, finding a job is your full-time job. This means combing through websites (such as seek, your university bulletin boards, social media, other industry webpages (eg. physiohub). If this doesn’t come up with the job you want googling can be your best friend. |  |
Getting your foot in the door
Resume Writing
 | Writing a resume is a skill in its own right. You can find tons of information on how to write a resume, with many sites having different opinions on the best way to grab an employers attention. Remember, part of writing a great resume is having it stand out. |
InterviewsYou’ve made a killer resume and applied to a few positions and actually heard back! The interview process can be stressful, especially when you have to compete with other classmates for the same positions. The larger companies will usually have a more standardized, HR-approach to interviews. It could be a formal, panel, or practical interview, or a combination of each. These companies tend to be hiring employees instead of independent contractors. Fortunately, smaller and less professional clinics sometimes only do a sit-down interview and may skip the practical portion. They may ask you a couple of PT-related questions to evaluate your clinical reasoning; however it is still in your best interest to be prepared for any practical questions. The bottom-line is if you are invited to an interview, you likely meet the required skill level. The interview is necessary to see if you can hold a conversation, fit the culture, and be able to generate business for the clinic. |  |
CLICK HERE FOR OUR
NEW GRAD GUIDE TO PRIVATE PRACTICE PHYSIOTHERAPY 2
News
We have even more free info! Scroll down to the bottom and filter results by 'Categories'
Archives
November 2023
July 2023
January 2023
November 2022
December 2021
November 2021
October 2021
September 2021
April 2020
March 2020
February 2020
January 2020
Categories
All
Ankle
Core
Exercise
Feet
Hamstrings
Injury Information
Knees
Low Back Pain
Physio Graduates
Planks
Posture
Running
Sports
 RSS Feed
RSS Feed