
Home Screening for Scoliosis - 5 Tips
Treating scoliosis is a race against gravity.
What is Scoliosis
Scoliosis was originally a Greek word meaning curved or bent. Today we use the word to one of the most common types of spinal curvatures. Scoliosis is simply a descriptive term, like headache, and not a precise diagnosis.
When a scoliosis develops the spine bends and rotates along its vertical axis causing an asymmetry of the spine and axial skeleton. These changes have cosmetic and physiological effects with long-term consequences which may result in significant health problems with severe curves.
Types of Scoliosis
There are many causes of scoliosis, like there are many causes of headache. The hardest part is determining which type of scoliosis the patient has.
Idiopathic Scoliosis
The word idiopathic also comes from the Greek language and means pathology unto itself. More simply, idiopathic means a condition not associated with any other disease or disorder. Unfortunately the term idiopathic is widely used in medical literature to indicate the cause of a given condition is unknown.
There are three main types of idiopathic scoliosis which are classified according to the age of onset.
INFANTILE – A curvature that develops before a child is two years old. Nine out of ten of these curves will spontaneously resolve. This type of scoliosis is very rare in Australia.
JUVENILE IDIOPATHIC – A curve that develops in the age range of two to ten years. This type is also rare in this country.
ADOLESCENT IDIOPATHIC SCOLIOSIS (AIS) – This type appears in early adolescence and is much more common in girls than boys. While the incidence of very small curves is similar in both sexes, the ratio of boys to girls for curves in the treatment category is 1 : 8-10. AIS in girls accounts for about 90 percent of curves seen in clinical practice.
The above remains a useful way of considering scoliosis. However, the following is a newer classification system:
EARLY/LATE ONSET SCOLIOSIS - It is rare for children to develop scoliosis below the age of 10. Given that scoliosis is driven by growth, one occurring in younger children is more likely to need treatment than those seen in adolescence. Early onset scoliosis is defined as that presenting at 5 years or less. Late onset is in those over 5 years. At 5 years or less, a scoliosis can have a major impact on health if untreated. This is because a deformed spine can affect the development of heart and lungs. Long term, this can lead to breathing and blood pressure problems (pulmonary hypertension) in adulthood. A scoliosis developing over the age of 5 does not significantly impact on heart and lung development. Life expectancy is generally normal.
The difficulty of treating scoliosis in the young is controlling the scoliosis without interfering with growth of the spine. In adolescents, surgery involves fusing the bent part of the spine. This straightens it and prevents further growth at those levels. This is not a problem as the spine has grown enough by that age. In fact, by the age of 10, the spine is 80 per cent grown.
Treatment in children aims at avoiding fusion (except in special circumstances).
Screening For Scoliosis
Where properly conducted school screening programs are carried out these should be supported and participation encouraged. School screening is best performed in girls in Years 7 and 9 (11 and 13 years of age). The Spine Society of Australia recommends that if screening is to be restricted on budgetary grounds, it should be limited to girls in Year 7. No case has ever been made for the routine screening of boys.
A two-tier screening process is recommended, the first being by school nurses trained in the Forward Bend Test (FBT - see below). Confirmation of a structural scoliosis by a doctor should take place before a family is notified. Over-diagnosis, a pitfall in screening programs, is best avoided by this two-tier approach. The notification rate should be less than three percent.
The abandonment of school screening programs led to the introduction of the National Self-Detection Program for Scoliosis. This entails the distribution of a brochure to girls in Years 7 and 9 via the school systems. The thrust of this approach is to place responsibility for curve detection on the adolescent population and for management of minor curves on the family doctor. Over-referral to specialists is to be avoided. Most curves do not require active treatment.
The Forward Bend Test
This is the key to the detection of scoliosis and it demonstrates the fixed rotatory component of a curve. In the thoracic region the ribs follow the rotating spine and move posteriorly and upwards, giving a prominence on the side of the apex - a right thoracic curve will have a right thoracic prominence in the FBT. In the lumbar region there are no ribs so with a lumbar
curve the muscles on the side of the apex become more prominent. This is called the bolster sign because of the appearance of the prominence being similar to that of a long pillow (bolster). The prominence with thoracolumbar curves is a mixture of the above two described findings Figure 2 demonstrates a correctly performed FBT in the girl shown in Figure 1.
First and foremost patients with AIS and their parents must understand that the diagnosis of AIS is a clinical and radiological one. The diagnosis is one of exclusion, that is the exclusion of those conditions such as neuromuscular disorder etc which can produce a curve. There are no biochemical or other markers (blood tests) specific for AIS. Further, there are no markers which will allow a spinal surgeon to predict accurately whether or not a given curve will progress. However, there are sound data on the probability (the risk) or progression as detailed in Table 1.
What is Scoliosis
Scoliosis was originally a Greek word meaning curved or bent. Today we use the word to one of the most common types of spinal curvatures. Scoliosis is simply a descriptive term, like headache, and not a precise diagnosis.
When a scoliosis develops the spine bends and rotates along its vertical axis causing an asymmetry of the spine and axial skeleton. These changes have cosmetic and physiological effects with long-term consequences which may result in significant health problems with severe curves.
Types of Scoliosis
There are many causes of scoliosis, like there are many causes of headache. The hardest part is determining which type of scoliosis the patient has.
Idiopathic Scoliosis
The word idiopathic also comes from the Greek language and means pathology unto itself. More simply, idiopathic means a condition not associated with any other disease or disorder. Unfortunately the term idiopathic is widely used in medical literature to indicate the cause of a given condition is unknown.
There are three main types of idiopathic scoliosis which are classified according to the age of onset.
INFANTILE – A curvature that develops before a child is two years old. Nine out of ten of these curves will spontaneously resolve. This type of scoliosis is very rare in Australia.
JUVENILE IDIOPATHIC – A curve that develops in the age range of two to ten years. This type is also rare in this country.
ADOLESCENT IDIOPATHIC SCOLIOSIS (AIS) – This type appears in early adolescence and is much more common in girls than boys. While the incidence of very small curves is similar in both sexes, the ratio of boys to girls for curves in the treatment category is 1 : 8-10. AIS in girls accounts for about 90 percent of curves seen in clinical practice.
The above remains a useful way of considering scoliosis. However, the following is a newer classification system:
EARLY/LATE ONSET SCOLIOSIS - It is rare for children to develop scoliosis below the age of 10. Given that scoliosis is driven by growth, one occurring in younger children is more likely to need treatment than those seen in adolescence. Early onset scoliosis is defined as that presenting at 5 years or less. Late onset is in those over 5 years. At 5 years or less, a scoliosis can have a major impact on health if untreated. This is because a deformed spine can affect the development of heart and lungs. Long term, this can lead to breathing and blood pressure problems (pulmonary hypertension) in adulthood. A scoliosis developing over the age of 5 does not significantly impact on heart and lung development. Life expectancy is generally normal.
The difficulty of treating scoliosis in the young is controlling the scoliosis without interfering with growth of the spine. In adolescents, surgery involves fusing the bent part of the spine. This straightens it and prevents further growth at those levels. This is not a problem as the spine has grown enough by that age. In fact, by the age of 10, the spine is 80 per cent grown.
Treatment in children aims at avoiding fusion (except in special circumstances).
Screening For Scoliosis
Where properly conducted school screening programs are carried out these should be supported and participation encouraged. School screening is best performed in girls in Years 7 and 9 (11 and 13 years of age). The Spine Society of Australia recommends that if screening is to be restricted on budgetary grounds, it should be limited to girls in Year 7. No case has ever been made for the routine screening of boys.
A two-tier screening process is recommended, the first being by school nurses trained in the Forward Bend Test (FBT - see below). Confirmation of a structural scoliosis by a doctor should take place before a family is notified. Over-diagnosis, a pitfall in screening programs, is best avoided by this two-tier approach. The notification rate should be less than three percent.
The abandonment of school screening programs led to the introduction of the National Self-Detection Program for Scoliosis. This entails the distribution of a brochure to girls in Years 7 and 9 via the school systems. The thrust of this approach is to place responsibility for curve detection on the adolescent population and for management of minor curves on the family doctor. Over-referral to specialists is to be avoided. Most curves do not require active treatment.
The Forward Bend Test
This is the key to the detection of scoliosis and it demonstrates the fixed rotatory component of a curve. In the thoracic region the ribs follow the rotating spine and move posteriorly and upwards, giving a prominence on the side of the apex - a right thoracic curve will have a right thoracic prominence in the FBT. In the lumbar region there are no ribs so with a lumbar
curve the muscles on the side of the apex become more prominent. This is called the bolster sign because of the appearance of the prominence being similar to that of a long pillow (bolster). The prominence with thoracolumbar curves is a mixture of the above two described findings Figure 2 demonstrates a correctly performed FBT in the girl shown in Figure 1.
First and foremost patients with AIS and their parents must understand that the diagnosis of AIS is a clinical and radiological one. The diagnosis is one of exclusion, that is the exclusion of those conditions such as neuromuscular disorder etc which can produce a curve. There are no biochemical or other markers (blood tests) specific for AIS. Further, there are no markers which will allow a spinal surgeon to predict accurately whether or not a given curve will progress. However, there are sound data on the probability (the risk) or progression as detailed in Table 1.
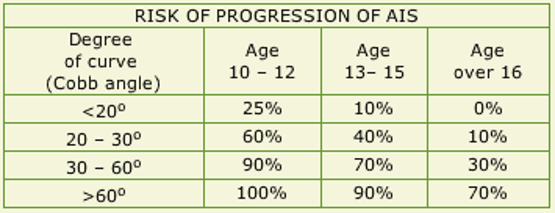
Data generated by the Scoliosis Research Society, Chicago, Illinois,USA
It is readily deduced from this table that curves are most likely to progress and require active treatment (bracing or surgery) the larger the curve is at presentation and the age at which medical advice is first sought. This is because curves progress most rapidly during the growth spurt – 11-13 years in girls and about 18 months later in boys. These are average figures and averages only appear on paper.
If you catch it early enough, the right exercises and treatment can help reduce if not eliminate the curves not to negligible levels.
Unfortunately, many cases aren’t spotted until the spinal curve is moderately advanced. At that point treatment becomes more difficult and the risk of progression increases threefold.
For kids with scoliosis, early prevention is critical. Despite the fact that the condition around 3-4 percent of the population(approx. 720,000 in australia), scoliosis screening remains deficient in the Australia.
Effective scoliosis treatment involves retraining the brain to correct the spine’s alignment; through involuntary exercises, kids can build new subconscious muscle memory and automatic habits to support a straighter spine. Children who start their neuromuscular retraining before the curve reaches 20 degrees can ultimately reduce its severity to less than 10 degrees.
Consider performing a home scoliosis test if you believe your child is at risk of developing the condition. Scoliosis is most likely to afflict:
If you catch it early enough, the right exercises and treatment can help reduce if not eliminate the curves not to negligible levels.
Unfortunately, many cases aren’t spotted until the spinal curve is moderately advanced. At that point treatment becomes more difficult and the risk of progression increases threefold.
For kids with scoliosis, early prevention is critical. Despite the fact that the condition around 3-4 percent of the population(approx. 720,000 in australia), scoliosis screening remains deficient in the Australia.
Effective scoliosis treatment involves retraining the brain to correct the spine’s alignment; through involuntary exercises, kids can build new subconscious muscle memory and automatic habits to support a straighter spine. Children who start their neuromuscular retraining before the curve reaches 20 degrees can ultimately reduce its severity to less than 10 degrees.
Consider performing a home scoliosis test if you believe your child is at risk of developing the condition. Scoliosis is most likely to afflict:
- Kids ages eight to 14.
- Girls, who are eight times more likely to get scoliosis than boys.
- Those with a thin or lanky body shape.
- A child whose parent or sibling has scoliosis.
- To conduct a scoliosis home screening, perform the following steps with your child.
STEP 1: Forward Bend
Doctors and school nurses routinely use this simple exam during scoliosis screenings. Have your child stand with arms extended and palms held together, then bend at the waist as if touching their toes. Examine the back both from behind and from the front, looking for any signs of asymmetry.
• Is one side of the rib cage higher than the other?
• Is the lower back uneven?
• Does one hip appear higher than the other?
STEP 2: Standing Straight
Changes in posture are one of the earliest warning signs of scoliosis—often they hint at the condition before the curve itself becomes visible. As the spine grows into its curve, the shoulders, waist and hips are thrust out of alignment. Have your child stand up straight while you inspect their posture from the front, from behind and from the side.
• Is one shoulder higher than the other?
• Is one arm farther away from the body?
• Is one shoulder blade higher than the other?
• Are the hips uneven?
• Does the back look too rounded?
STEP 3: Clothes Check
Subtle changes in posture can be hard to spot, but sometimes your child’s clothing provides the first visible indication of spinal curvature. During your scoliosis home screening, study your child for signs of ill-fitting or uneven clothing.
• Is the hemline uneven?
• Does one pant leg hang lower than the other?
• Does one shirtsleeve appear longer than the other?
STEP 4: Eyes and Ears
The alignment of your child’s eyes and ears can also signal a spinal abnormality. Examine your child’s eye line and ears to check for scoliosis red flags.
• Is the eye line tilted?
• Is the center of the eyes out of alignment with the center of the hips?
• Is the inner ear forward of the shoulder?
STEP 5: Taking a Walk
Scoliosis can sometimes cause a slight limp or other irregularities while walking. Study your child’s normal gait to determine if any of these signs are present.
• Does your child have a slight limp?
• Does the body tilt to one side?
• Does one leg seem shorter than the other?
Doctors and school nurses routinely use this simple exam during scoliosis screenings. Have your child stand with arms extended and palms held together, then bend at the waist as if touching their toes. Examine the back both from behind and from the front, looking for any signs of asymmetry.
• Is one side of the rib cage higher than the other?
• Is the lower back uneven?
• Does one hip appear higher than the other?
STEP 2: Standing Straight
Changes in posture are one of the earliest warning signs of scoliosis—often they hint at the condition before the curve itself becomes visible. As the spine grows into its curve, the shoulders, waist and hips are thrust out of alignment. Have your child stand up straight while you inspect their posture from the front, from behind and from the side.
• Is one shoulder higher than the other?
• Is one arm farther away from the body?
• Is one shoulder blade higher than the other?
• Are the hips uneven?
• Does the back look too rounded?
STEP 3: Clothes Check
Subtle changes in posture can be hard to spot, but sometimes your child’s clothing provides the first visible indication of spinal curvature. During your scoliosis home screening, study your child for signs of ill-fitting or uneven clothing.
• Is the hemline uneven?
• Does one pant leg hang lower than the other?
• Does one shirtsleeve appear longer than the other?
STEP 4: Eyes and Ears
The alignment of your child’s eyes and ears can also signal a spinal abnormality. Examine your child’s eye line and ears to check for scoliosis red flags.
• Is the eye line tilted?
• Is the center of the eyes out of alignment with the center of the hips?
• Is the inner ear forward of the shoulder?
STEP 5: Taking a Walk
Scoliosis can sometimes cause a slight limp or other irregularities while walking. Study your child’s normal gait to determine if any of these signs are present.
• Does your child have a slight limp?
• Does the body tilt to one side?
• Does one leg seem shorter than the other?
A scoliosis home screening is one of the most effective ways to detect the condition early. As a parent, you know your child better than anyone. If you spot any of the above warning signs, have your child’s posture examined by a specialist.